


Wealthier people have a lot of advantages when it comes to health care; they are more likely to have insurance, more likely to have access to specialty care, and on average live longer and healthier. But do rich patients get better value of care?
The rates at which patients receive “high-value” care (services that improve outcomes and reduce cost in the long run) and avoid “low-value” care (services that are wasteful, with little or no clinical benefit) could have a big impact on overall health.
New study measures high and low-value care by income
In a recent study in Health Affairs, researchers Sungchul Park at Korea University and Rishi K. Wadhera at Beth Israel Deaconess Medical Center in Boston, MA examined the relationship between patient income and their receipt of certain high-value or low-value services.
Using data from the 2010–19 Medical Expenditure Panel Survey (MEPS), the authors compared rates of eight high-value and nine low-value services among patients by income. High-value services included certain cancer screenings, blood pressure measurement, cholesterol measurement, influenza vaccine, and diabetes care measures. Low-value services included antibiotics for cold and flu, benzodiazepine for depression, opioids for back pain or headache, NSAIDs for non-recommended conditions, and certain imaging for back pain or headache.
Income was categorized by less than 200% of the federal poverty level, 200-400%, and 400% or more based on family income. Results were also separated by age as most older adults (65+) are covered by Medicare. Researchers controlled for race, sex, census region, insurance coverage, and other patient characteristics.
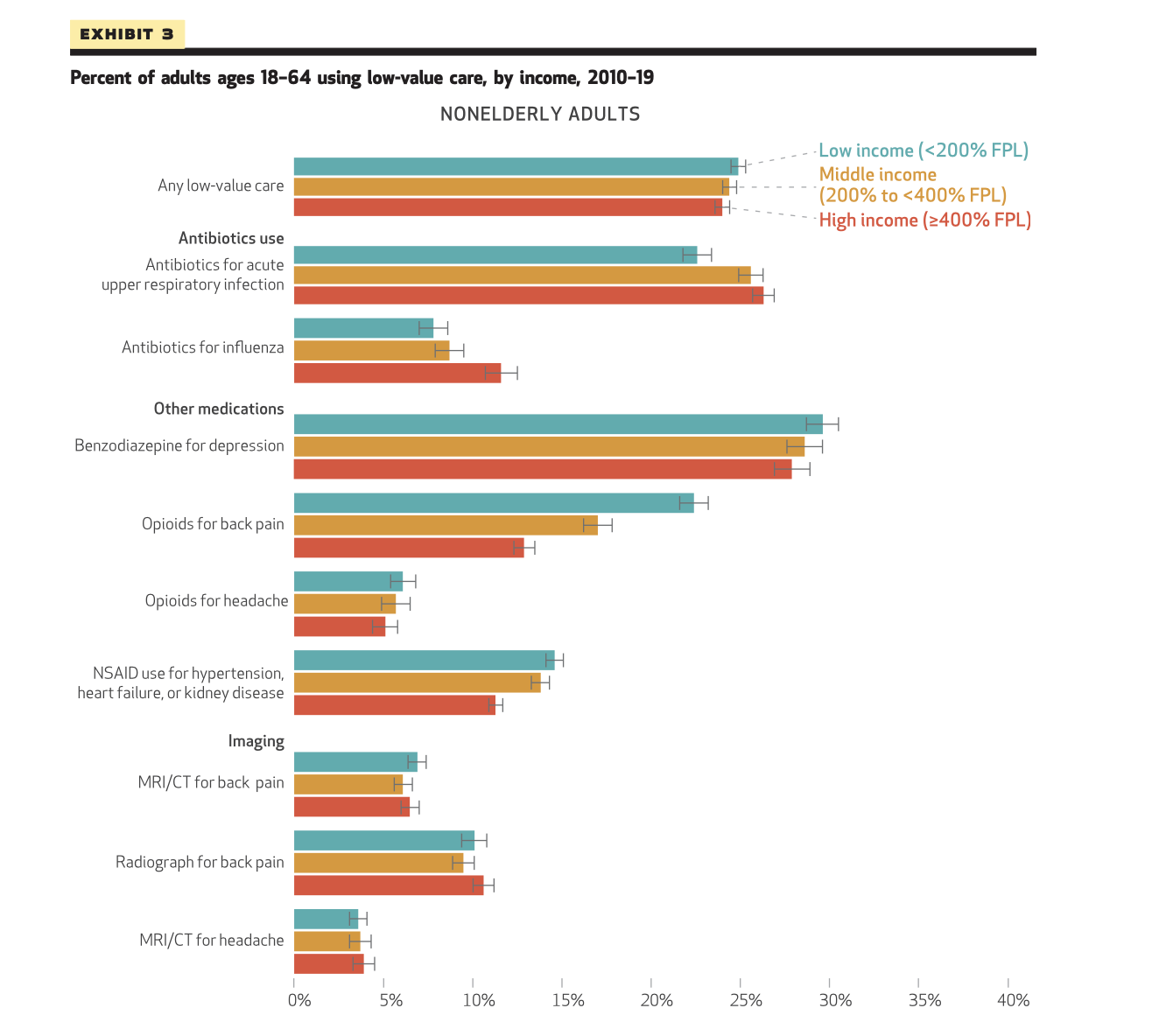
Rich patients get more high-value care, but also get more low-value antibiotics
The study authors found that high-income adults were more likely to receive high-value services, especially in the group of younger (<65) adults. For example, high-income younger patients had rates of colorectal cancer screening nearly 20 percentage points higher than low-income patients.
Overuse was prevalent among all categories of patients in the study, with about a quarter of patients receiving at least one low-value service. However, unlike with high-value care, the association with overuse and income was mixed. High-income patients had higher rates of some low-value services, but lower rates for others.
For example, high-income patients were more likely to get antibiotics for cold and flu than low-income patients. Antibiotics for these conditions are not only ineffective, but expose patients to the risk of gastrointestinal symptoms and antibiotic-resistant infections. High-income older adults were also more likely to receive low-value prostate cancer and cervical cancer screenings, which can lead to false positives and overtreatment.
However, low-income patients were more likely to receive other types of low-value medications, such as opioids for back pain, benzodiazepines for depression, and NSAIDs for non-recommended uses. Benzodiazepines for depression were the most common type of overuse, with nearly 30% of low-income adults in the study receiving this treatment.
Opioids for back pain had the biggest variation based on income in the younger adult group; about 23% of low-income adults received opioids for back pain, compared to about 13% for high-income patients. These rates of overmedication are concerning, as opioids for back pain can lead to physical dependence, and benzodiazepine overuse can lead to debilitating withdrawal symptoms.
Behind the variation
What could explain these differences in high and low-value care by income? Although the authors accounted for patient differences in insurance status and education, there are many other mechanisms that can impact our quality of care. The authors cite “health care provider shortages, long distances to health care facilities, and limited access to transportation in low-income communities” that may reduce their receipt of high-value care.
Cost is also a likely factor. Even for patients with insurance, out-of-pocket costs can be prohibitive. For example, the cost of preventive colon cancer screening is supposed to be covered in full, but if pre-cancerous polyps are found, the colonoscopy can be billed as a “diagnostic” test, which can cost patients thousands of dollars. With surprise bills popping up everywhere, it’s no wonder people may avoid preventive screenings, even those recommended by their doctor.
Patient behavior or provider perceptions can impact receipt of low-value care. Providers may prescribe low-value antibiotics to high-income patients more because these patients are more likely to ask for them, or because providers worry that not doing so will impact their patient satisfaction scores.
Lastly, variation in provider practices also play a role. Research from the Lown Institute and others shows that rates of low-value services vary widely among hospitals and health systems. If low-income patients are more likely to go to certain hospitals (which is often the case in segregated hospital markets) and these hospitals deliver more low-value care, that could explain some of the differences. (See how your local hospital performs on avoiding common low-value services!)
The fact that rich patients were more likely to receive every type of high-value care measured reflects issues of access in our health system. We need universal coverage with low or no cost sharing so that preventive care is truly affordable for all. On the overuse side, there’s still a lot we don’t know about what causes different rates of low-value services by income. The study authors recommend more research “to gain a better understanding of these mechanisms to develop policies and interventions that encourage the use of high-value care and discourage the use of low-value care across all income levels.”