


Nonprofit hospitals are required to have offer free or discounted care for uninsured patients or those unable to pay, and to codify their rules around these discounts in a financial assistance policy (FAP). However, most states do not have minimum requirements for how hospitals implement their FAPs, which means that these policies can be wildly different depending on the hospital.
Amid increased scrutiny on hospital billing and collections practices, one would expect hospitals to make their FAPs more generous. However, when it comes to financial assistance policies, change is not always for the better, a new study of hospital FAPs in the Journal of General Internal Medicine finds.
Why financial assistance policies matter
Medical debt is prevalent in the U.S., with at least 8% of Americans and as many as 41% reporting medical debt for themselves or a family member. Given the high cost of medical care, insurance coverage gaps and high deductibles, and limited ability to weather financial crises, having access to financial assistance from hospitals can be the difference between families going into debt or not.
The Affordable Care Act requires nonprofit hospitals to have a FAP, make it publicly available, and refrain from taking extraordinary debt collection actions before determining FAP eligibility. However, there is no federal requirement for a minimum level of financial assistance hospitals must provide. As a result, eligibility requirements and available discounts vary considerably across US hospitals.
For example, one hospital might offer free care to anyone making up to 400% of the federal poverty level, while another may only offer the same discount to patients making only 100% of the federal poverty level. These differences can occur even for hospitals in the same cities.
An update on hospital policies
To understand differences in hospital FAPs and changes over time, Dr. Christopher Goodman at the University of South Carolina School of Medicine and colleagues have been tracking a sample of FAPs. In 2022, they released an analysis of FAPs at large acute care hospitals between 2019 and 2021. They found that 56% of policy changes made FAPs more generous, 19% were more restrictive, and 25% had unclear impact.
Now, Goodman and colleagues have published another update on their hospital sample, tracking hospital FAP changes from 2021-2023. They found that the plurality of hospitals (30%) made changes that were considered “more generous,” such as expanding their income thresholds for assistance to include more people, making patients automatically eligible for assistance, and expanding assistance to underinsured patients. However, the authors noted that income threshold expansions were small and likely not enough to cover inflation or cost of living changes from recent years.
A smaller proportion of hospitals (6%) added restrictions to their FAPs, such as additional residency requirements, reduced income thresholds for discounts, or restricting financial assistance to uninsured patients.
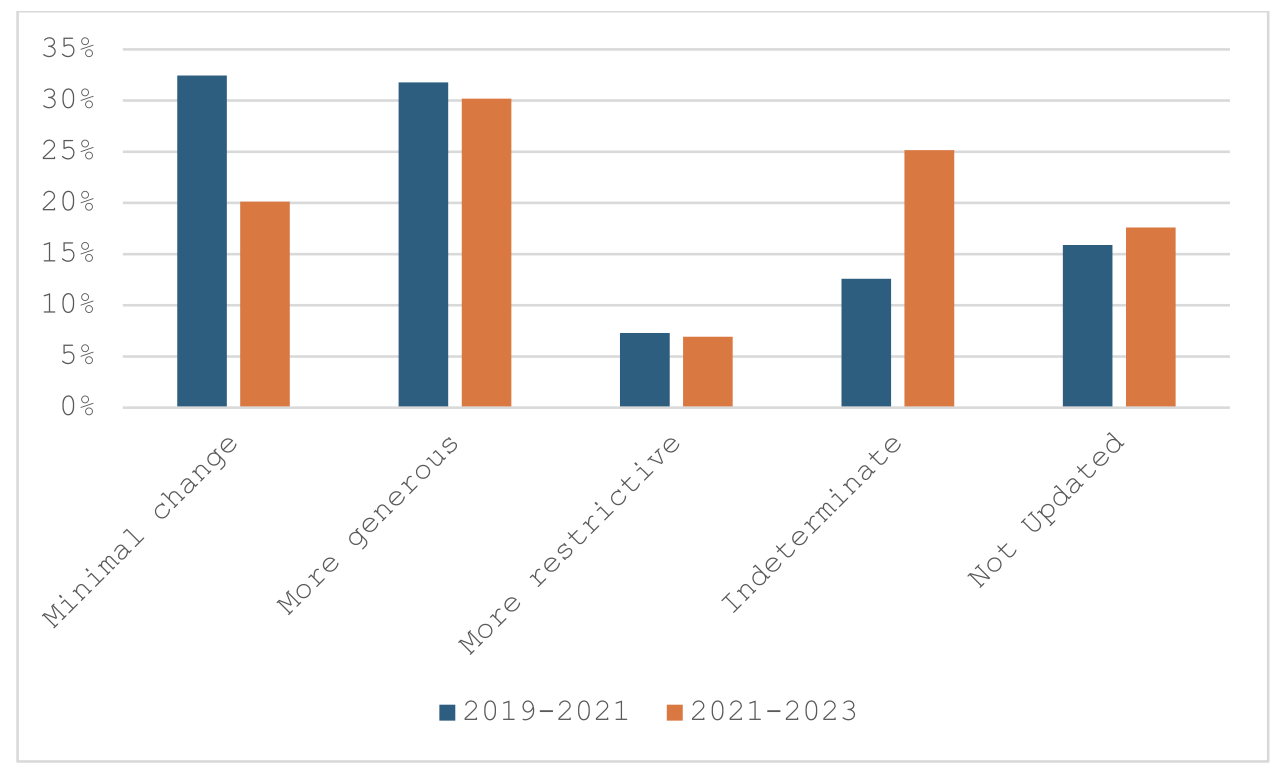
Compared to the previous time period, many more hospitals made changes that have an “indeterminate” effect, rather than being clearly positive or negative. Common examples of these changes were moving content on financial assistance to a different policy, mentioning external vendors used to determine eligibility, and unclear changes to asset thresholds for assistance. (As previous research from Dr. Goodman and the Lown Institute’s Kelsey Chalmers found, use of third party tools for patient screening can have a positive or negative effect on relieving medical debt, depending on how hospitals use these tools.) Overall these types of “indeterminate” changes create more complexity and less transparency, making it increasingly difficult for patients to understand the policy and access assistance.
To learn more on this important topic, the Lown Institute is collecting data on hospital billing and collection practices for 2,500 hospitals. Download the data and read more about this project!