


For frail older adults, taking several blood pressure medications can lead to dizziness, falls, and other adverse drug events, making this medication a potentially good one to deprescribe (discontinue or reduce the dose). However, clinicians or family members may avoid deprescribing a blood pressure medication because they fear that patients’ blood pressure will rise dangerously. For those who are uneasy about deprescribing hypertension medications for older adults, the OPTIMISE trial results may put their mind at ease.
The recently-published Optimising Treatment for Mild Systolic Hypertension in the Elderly (OPTIMISE) study is a randomized controlled trial of 569 patients, conducted in 69 primary care sites across England. Participants were at least 80 years old, had controlled blood pressure, and were taking at least two antihypertensive medications, making them good candidates for deprescribing. Patients were randomized to either deprescribe one blood pressure medication, or continue with usual care. Patients were monitored for about three months, so this trial shows short-term effects of deprescribing, but not long-term effects.
The trial leaders wanted to know whether taking away one blood pressure medication would result in dangerous increases in blood pressure, or if patients who deprescribed could still keep their blood pressure under control. They also measured changes in frailty, quality of life, and adverse effects between the intervention and control groups. Here are a few takeaways:
Blood pressure stayed under control, even with deprescribing
This trial was designed as a “noninferiority” trial, to measure whether deprescribing could be as effective as controlling blood pressure as usual care. The researchers found that after 12 weeks, 86.4% of patients in the deprescribing group and 87.7% of patients in the control group still had their blood pressure under control, which was within the level of relative risk pre-specified by the researchers. These results suggest that many older frail patients can reduce their blood pressure medications and still keep their blood pressure under control.

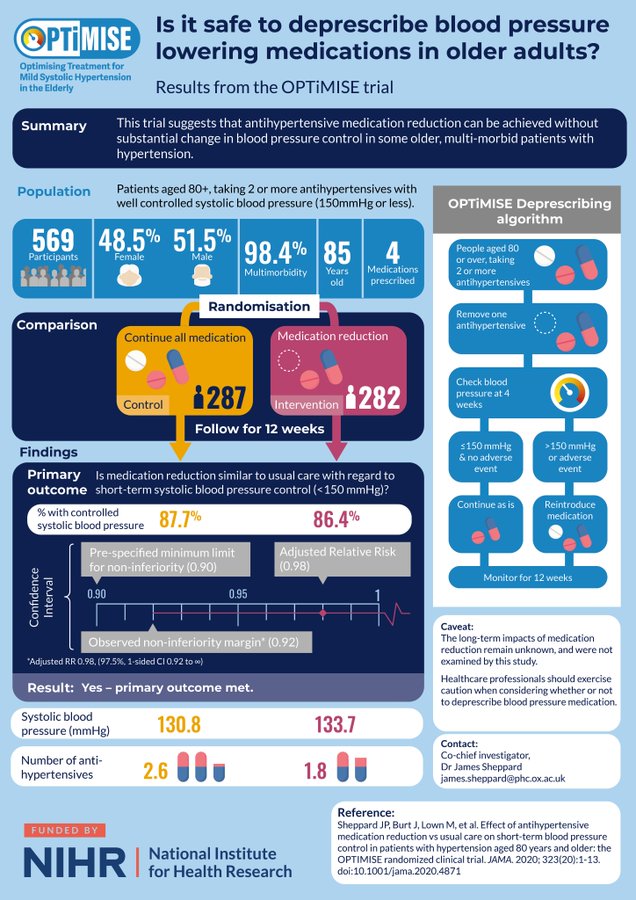
The authors also measured difference in mean blood pressure levels between the intervention and control group. The deprescribing group had mean systolic blood pressure of 133.7 while the control group had slightly lower blood pressure of 130.8, a difference of 3.4mm HG.
How much does this difference in blood pressure matter? This question is especially fraught, as the target for what should be seen as “normal” blood pressure in the US has changed several times, and is still under debate. Some clinicians argue that even a small increase in blood pressure is not desirable, and that lower is better, even for old and frail patients. “Although this absolute difference may seem minimal, such differences in BP can potentially lead to long-term differences in outcomes at the population level,” wrote professors Dr. Eric Peterson and Dr. Michael Rich in an accompanying editorial in JAMA. (It is worth noting that Dr. Peterson reported receiving personal fees from several drug companies in his disclosure of financial conflicts including Cerner, Livongo, AstraZeneca, Janssen, and Amgen.)
Peterson and Rich cite the SPRINT trial from 2017 which found a 25% relative reduction in cardiovascular events for patients 65 and over with highly controlled blood pressure. However, other clinicians note that an aggressive approach to blood pressure control often leads to side effects, and that the harms of blood pressure drops may outweigh the benefits for older patients.
In the end, the importance of 3.4mm increase “depends on other risks, such as baseline blood pressure and patients’ preferences,” wrote Dr. Michael Steinman, Professor of Geriatatrics at UCSF and co-Principal Investigator of the US Deprescribing Research Network, on Twitter. For example, an increase from a systolic blood pressure of 130mm and 133mm may be acceptable for an older patient who wants to take fewer medications, but an increase of 148 to 151 may be too risky.
As well as blood pressure levels, researchers measured frailty, quality of life, and adverse effects between the intervention and control groups. None of these outcomes were significantly different between the two groups. However, the authors point out that they monitored patients for only 12 weeks; we need more research on the long-term impact of deprescribing compared to usual care.